OSCE -60 year old female with complaints of vomitings,pain abdomen since 10 days
This is an online e log book to discuss our patient de-identified health data shared after taking his / her / guardians signed informed consent. Here we discuss our individual patients problems through series of inputs from available global online community of experts with an aim to solve those patients clinical problem with collective current best evident based input.





 urine for ketone bodies-negative
urine for ketone bodies-negative
 serum osmolality-285m osm/kg
serum osmolality-285m osm/kg
 Troponin I -6.9pg/ml
Troponin I -6.9pg/ml
 spot urinary potassium-4.6
spot urinary potassium-4.6
 Serum electrolytes on 9/11
Serum electrolytes on 9/11
 rft on 9/11
rft on 9/11

hemogram on 11/11
 rft on 11/11
rft on 11/11

 rft on 12/11
rft on 12/11

 rft on 13/11
rft on 13/11

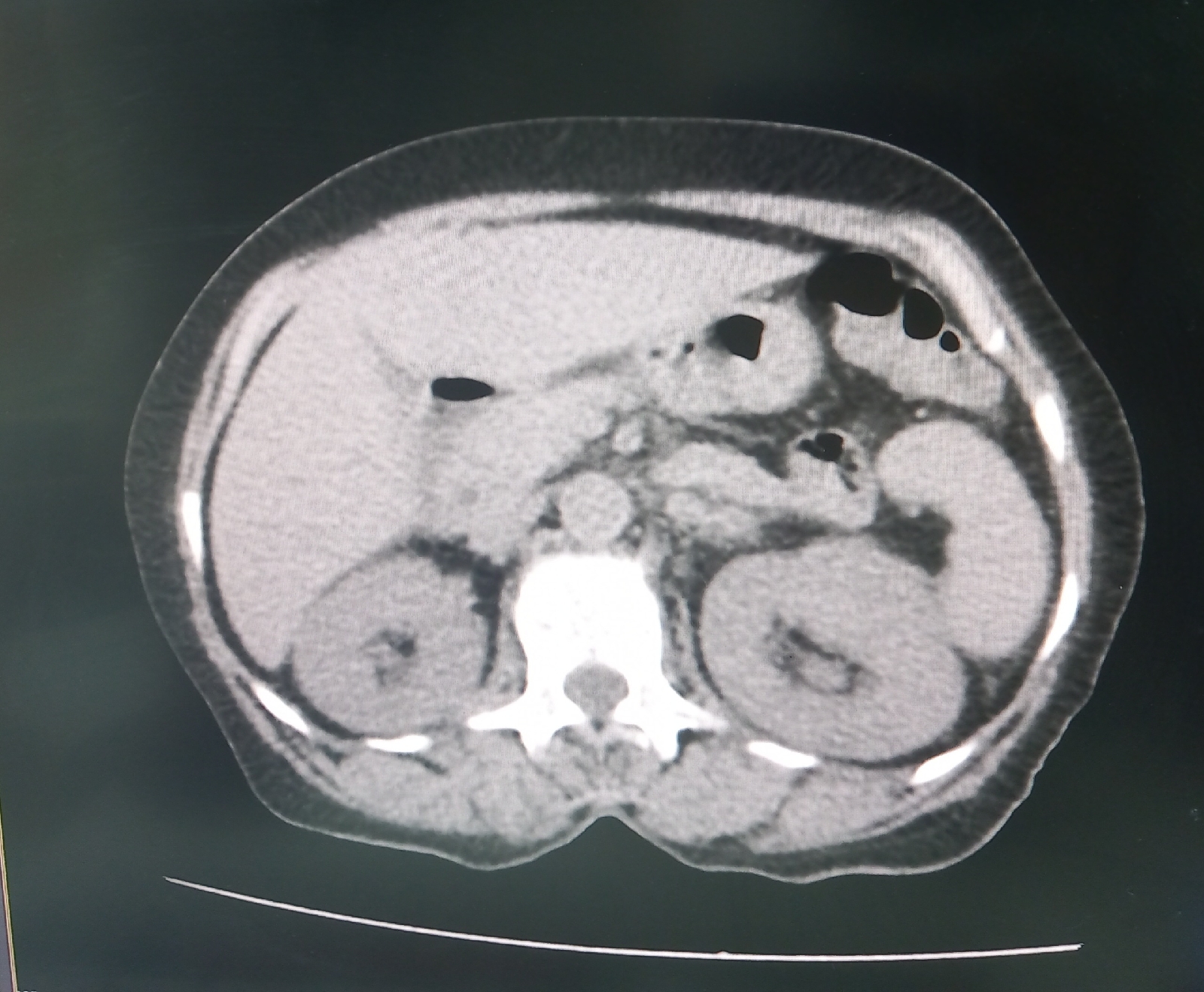
CT
 2d echoe
2d echoe
 urine for c/s -no growth seen
urine for c/s -no growth seen


USG- altered echotexture and increased AP diameter, increased vascularity of left kidney

This E blog also reflects my patient centered online learning portfolio and your valuable inputs on the comment box is welcome.
I have been given this case to solve in an attempt to understand the topic of " patient clinical data analysis" to develop my competency in reading and comprehending clinical data including history, clinical findings, investigations and come up with diagnosis and treatment plan
Chief complaints-
60 year old female patient came to casualty with complaints of vomitings since 10 days which is non bilious, non projectile, food particles as content.
C/O pain abdomen since 10 days,insidious onset, intermittent type of pain at left loin associated with giddiness since morning.
H/O increased urine output since 3 to 4 days ,increased frequency, increased urgency present.
H/O fever present
No H/O hematuria
No H/O pyuria
No H/O graveduria
No H/O previous renal surgeries
H/O constipation present.
N/H/O cold,cough,allergies.
N/H/O chest pain
Past History -
K/C/O DM type 2 since 5 months ,on irregular medication
No h/o Hypertension, asthma, tuberculosis, epilepsy ,CVA,CAD
Personal history
Appetite-Normal
Diet-Mixed
Bowels-Regular
Micturition-Increased urination
Allergies-No
Addictions-Alcohol -occasional
Family history-Not significant
General examination-
Patient is conscious, coherent and cooperative and well oriented to time place and person
No signs of,icterus,cyanosis,clubbing, lymphadenopathy
Pallor -present

Vitals -
Temp-102.9F
PR-102/MIN
BP-110/70MM HG
GRBS-416MG/DL
SYSTEMIC EXAMINATION
CVS-S1,S2 heard no murmurs
RS-BLAE ,NVBS
Abdomen-soft,tenderness present at left iliac region
No organomegaly
Bowel sounds-Present
CNS-NFD
Investigations
Urinary chloride-196mmol/l
Spot urinary sodium -42mmol/l
FBS-236mg/dl
Hba1c-7.5%
Hemogram on 9/11
Serology -Negative
hemogram on 11/11
Hemogram on 12/11
Hemogram on 13/11
CT
Blood for c/s-no growth seen
Chest x ray
USG- altered echotexture and increased AP diameter, increased vascularity of left kidney
Impression-Left pyelonephritis
Diagnosis-k/C/O DM 2 with left pyelonephritis with dyselectrolemia
Inpu/output-2000/700ml on 9/11
Input/output -2150/750 ml on 10/11
GRBS
9/11/23
8am -250mg/dl -12units HAI,8 units nph
10am -248 mg /dl
2pm-115 -6 units HAI
8pm-177 no food taken
10pm -139
2am -134
10/11/23
8am -163 -6units HAI ,4units nph
10am-360mg/dl
4pm-133mg/dl
8pm-103mg/dl
2am-115mg/dl
11/11/23
8am-147-6units HAI,4units nph
10am -175
12pm-113-6units HAI
4pm-216
8pm-344-12units HAI 8units nph
12/11/23
2am-85
8am -107mg/dl -6units HAI,4 units nph
10am -161 mg /dl
2pm-225 -6units HAI
4pm-310
8pm-296-6units hai,4units nph given
10pm-183
13/11/23
12am-155
8am -146 6units HAI
4units nph
Treatment
1:Inj Neomol 1g IV sos if temp >101F
2:IV fluids NS at 100ml /hr
3:Inj Piptaz 4.5gm IV/TID
4:Inj HAI According to GRBS SC/TID(pre meal)
5:Inj -NPH according to GRBS SC/BD
6:Monitor vitals
7:GRBS monitoring
8:TAB dolo 650 mg PO/SOS
9:Inj Kcl 20meq in 500ml NS over 4 to 6 hours ×2 infusions
OSCE
Q.What are the symptoms and classic triad of pyelonephritis?
Ans-Pain at left loin region radiating to iliac fossa and suprapubic area
Tenderness and guarding in renal angle
H/O Increased urination associated with increased frequency and increased urgency
Burning micturition
Fever
Classic triad-loin pan,fever,tenderness over kidneys
Q.What are the investigations done to dignose pyelonephritis?
Ans-1.Hemogram-Show leucocytosis
2.Urine examination-
Microscopy shows pus cells and organisms
Urine C/S- shows growth of causative organism
3.Usg
4.CT
Q.Management of Acute pyelonephritis?
Ans-Intravenous antibiotics according to growth of organism
Q.What are the complications of pyelonephritis?
Ans.common in patient of diabetes mellitus or with urinary tract obstruction
Necrotising papillitis/papillary necrosis -More common in analgesic abuse nephropathy and in sickle cells disease
Pyonephrosis- rarely the abscesses in kidney in Acute pyelonephritis are extensive this results in inability of abscesses to drain and transforms kidney intlo multilocular sac filled with pus
Perinephric abscess-The abscesses in kidney may extend through capsule of kidney into perinephric tissue and form abscess
Q.What is the etiopathogenesis of Acute pyelonephritis?
Etiology- infection of lower uti
Mc organisms - E.coli ,Enterobacter,kliebsiella,Pseudmonas and proteus
Pathogenesis-
Ascending infection-Bacteria multiply in urinary bladder and produce asymptomatic bacteriuria and causes urethritis,cystitis ascend further up into ureter,extend into renal pelvis and then to renal cortex
Hematogenous infection-MC in immunocompromised patients
Q.What are the morphological features of pyelonephritis?
Gross- enlarged swollen kidney
C/S- small abscesses with heamorrhagic rim
Microscopic -Acute Inflammation involving interstitium and tubeles.shows large number of neutrophils .
Q.What are the radiological findings of pyelonephritis?
Usg- Altered echotexture and increased vascularity ,increase in size of kidney
CT-perinephric stranding present.,dilated collecting system.
SWOT analysis (Strengths, Weaknesses, Opportunities, Threats) of the patient's case:
Strength
She has good support from family
She recovered very soon with the medication
Weaknesses:
1. Her financial status
2. She is depressed about her disease
Opportunities:
1. Provision of free testing such as CECT


Comments
Post a Comment